Symptoms Are State Signals
Why patients need better ways to describe clinical change.
Find the change to understand progression
Patients often know something has changed before the system does
Many clinical changes begin quietly. Before a scan looks different, before a blood result is reviewed, before a clinician documents a new examination finding, the patient may already know that something has shifted.
The pain is not the same. The breathlessness is coming on earlier. The headache has changed pattern. The abdominal pain is now related to food. The chest tightness occurs with less exertion. The bowel symptoms are becoming more frequent. The arthritis pain is limiting walking more than it did last month.
These are not merely complaints. They are early signals of state change.
Healthcare often depends on these signals, but it does not always capture them well. Patients are commonly told to "keep a diary," "monitor symptoms," or "come back if things get worse." These instructions are familiar, and sometimes reasonable, but they are often too vague for the complexity of clinical change in real life.
A headache diary may record that headaches occurred, but not whether the character changed, whether aura appeared, whether medication response altered, whether sleep or food triggers mattered, or whether the pattern now requires escalation. A pain diary may record severity, but not location, radiation, onset, aggravating factors, functional impact, or red-flag features. A breathlessness diary may record that symptoms were present, but not exertional threshold, reliever response, nocturnal symptoms, sputum change, infection features, or activity limitation.
The problem is not that patients are poor historians. The problem is that patients are often not given enough structure.
They are asked to describe complex biological change using loose, unstructured language. They need better tools. They need a structured way to describe change.
Structure Improves the Patient's Own Clinical Language
A patient may begin with a simple sentence: "My stomach pain is worse." That statement matters, but it is incomplete.
With structure, the same patient may say:
"The pain is cramping, severe, in the right upper abdomen, starts after a fatty meal, lasts several hours, is associated with nausea, and is only partly relieved by analgesia."
That is a different clinical object. It gives location, nature, timing, trigger, duration, associated symptoms, and treatment response. It helps the clinician think about biliary pain, gastrointestinal causes, medication effects, and escalation risk.
A patient may initially say: "My chest feels tight."
With structure, that becomes:
"The tightness comes on when I walk uphill, lasts about five minutes, settles with rest, has become more frequent over the last two weeks, and now occurs with less exertion."
That is no longer a vague symptom. It may represent a change in cardiac risk state.
A patient may say: "My asthma is playing up."
With structure, that becomes:
"I am needing salbutamol four times per day, waking overnight with wheeze, coughing more, and walking less than usual because of breathlessness."
That gives a triage system, and the clinician reviewing the output, a clearer signal. It does not diagnose the patient. It improves the quality of the information reaching clinical judgement.
Structured symptom assessment does not replace the clinician. It improves the signal before the clinician receives it.
NILDOCARP: A Practical Scaffold for Symptom Description
One useful clinical scaffold is the mnemonic NILDOCARP:
| Element | Patient-facing question |
|---|---|
| Nature | What does it feel like? |
| Intensity | How severe is it? |
| Location | Where is it? |
| Duration | How long does it last? |
| Onset | How did it begin? |
| Offset | How does it settle? |
| Concomitant features | What else occurs with it? |
| Aggravating factors | What makes it worse? |
| Relieving factors | What improves it? |
| Precipitants | What seems to trigger it? |
This structure helps patients move from vague symptom language to clinically meaningful description. It can be used across many conditions:
- biliary colic
- renal colic
- migraine
- angina pectoris
- asthma
- inflammatory bowel disease flare
- osteoarthritis pain
- peripheral neuropathy
- multiple sclerosis relapse
- post-operative pain
- chronic pelvic pain
- abdominal pain syndromes
The same scaffold works because most symptoms and signs have a pattern. Pain has a nature, intensity, location, duration, onset, offset, aggravating factors, relieving factors, and triggers. Breathlessness has severity, timing, exertional threshold, associated symptoms, reliever response, and precipitating context.
Bowel symptoms have frequency, urgency, bleeding, pain, systemic features, food associations, medication response, and functional impact. Neurological symptoms have distribution, timing, progression, associated deficits, triggers, and recovery pattern.
The structure does not force every patient into the same story. It helps each patient notice what matters in their own story.
The Symptom Diary Should Become a Symptom State Record
Traditional symptom diaries are often too nebulous. They may ask the patient to record pain, headaches, bowel symptoms, or breathing difficulty, but without enough structure to recognise meaningful change.
A more useful symptom state record would capture:
| Dimension | What it helps capture |
|---|---|
| Symptom pattern | What the symptom is doing over time |
| Severity score | How intense it is, and whether that intensity is changing |
| Anatomical location | Where the symptom is, including spread or radiation |
| Timing | When it occurs, how long it lasts, and whether frequency is changing |
| Triggers and relieving factors | What makes it worse, what improves it, and what seems to precipitate it |
| Functional effect | How the symptom changes walking, sleep, work, self-care, or daily activity |
| Associated symptoms | What else occurs with it, including red-flag features |
| Medication response | What has been tried and whether the response is changing |
| Baseline comparison | How this differs from the patient's usual state |
| Escalation flags | Features that should change urgency, routing, or clinician review |
This is not just more data. It is better-shaped data.
For migraine, a structured record may include headache location, pulsating or pressure quality, severity, duration, aura, nausea, photophobia, sleep relationship, menstrual relationship, food triggers, medication use, medication response, neurological symptoms, and frequency trend.
For osteoarthritis, it may include joint location, relationship to load-bearing, morning stiffness duration, walking tolerance, sleep disruption, swelling, medication response, flare triggers, activity limitation, and functional goals.
For inflammatory bowel disease, it may include stool frequency, blood or mucus, abdominal pain, urgency, nocturnal symptoms, fever, weight loss, dietary associations, medication adherence, steroid response, and extraintestinal symptoms.
This is more precise than asking the patient to "keep a diary." It gives the patient a way to observe change, not just remember it later. It turns symptom tracking into structured, patient-facing state management.

State signals build the connection
Scores and Body Maps Make Symptoms Easier to Compare
Structured questions can be paired with visual tools. A visual analogue scale score allows the patient to record severity over time. The most useful part is not the single number. It is the trajectory.
A pain score of 7 out of 10 may be clinically relevant. But it becomes much more meaningful when compared with the patient's prior state:
- 3 out of 10 last week
- 7 out of 10 today
- 9 out of 10 overnight
- 4 out of 10 after medication
The same principle applies to breathlessness, fatigue, nausea, itch, dizziness, bowel urgency, sleep disturbance, and functional limitation. An anatomical map adds another layer. It allows the patient to mark where symptoms occur and how they move.
This is useful for radicular pain, renal colic, biliary pain, chest pain, migraine, neuropathy, arthritis, abdominal pain, dermatological symptoms, and post-operative symptoms. A mark on a body map can show distribution, radiation, spread, laterality, and change over time.
When combined with structured questions, the symptom becomes a richer clinical state object. It is still the patient's subjective experience. But it is now described in a way that can be followed, compared, and clinically interpreted.
Structured Symptoms Support Safer Triage
Regenemm Triage can use structured symptom assessment to help identify risk, urgency, and appropriate routing. A virtual nurse or virtual doctor should not have to infer risk from vague text alone. It should guide the patient through a disciplined symptom description, then present the resulting state evidence in a clinically useful way.
For chest pain, the relevant questions may include:
- Is it exertional?
- Does it settle with rest?
- Is it increasing in frequency?
- Is it associated with shortness of breath, sweating, nausea, syncope, or radiation?
- Is there known ischaemic heart disease?
- Is this different from baseline?
For asthma, the system needs to know:
- Is there breathlessness at rest?
- Is the patient waking at night?
- Is reliever use increasing?
- Is speech limited?
- Is there poor response to bronchodilator?
- Are there infection features?
For renal colic, the system should identify concerning features such as fever, vomiting, known solitary kidney, uncontrolled pain, reduced urine output, pregnancy, or significant comorbidity.
For inflammatory bowel disease flare, it should look for bleeding, fever, dehydration, severe abdominal pain, weight loss, steroid dependence, immunosuppression, and extraintestinal symptoms.
The point is not to make uncontrolled autonomous decisions. The point is to stratify state, identify concerning patterns, preserve uncertainty, and support appropriate routing.
From Patient Experience to Governed Clinical Signal
Symptoms are subjective. That does not make them weak. But they are initially very unstructured.
In medicine, subjective experience is often the earliest evidence that something has changed. Pain, breathlessness, dizziness, fatigue, nausea, weakness, numbness, bowel urgency, visual disturbance, and sleep disruption all matter because they tell us how the patient's state is changing in real life.
The challenge is to preserve the patient's experience while making it clinically usable. That requires structure: symptom scaffolds, severity scores, anatomical maps, comparison with baseline, associated features, medication response, escalation flags, and time-based trends.
This is where patient-facing AI becomes clinically meaningful. It should not simply collect free text and produce a summary. It should help the patient describe change more clearly, then convert that description into governed state evidence for review, triage, and care co-ordination.
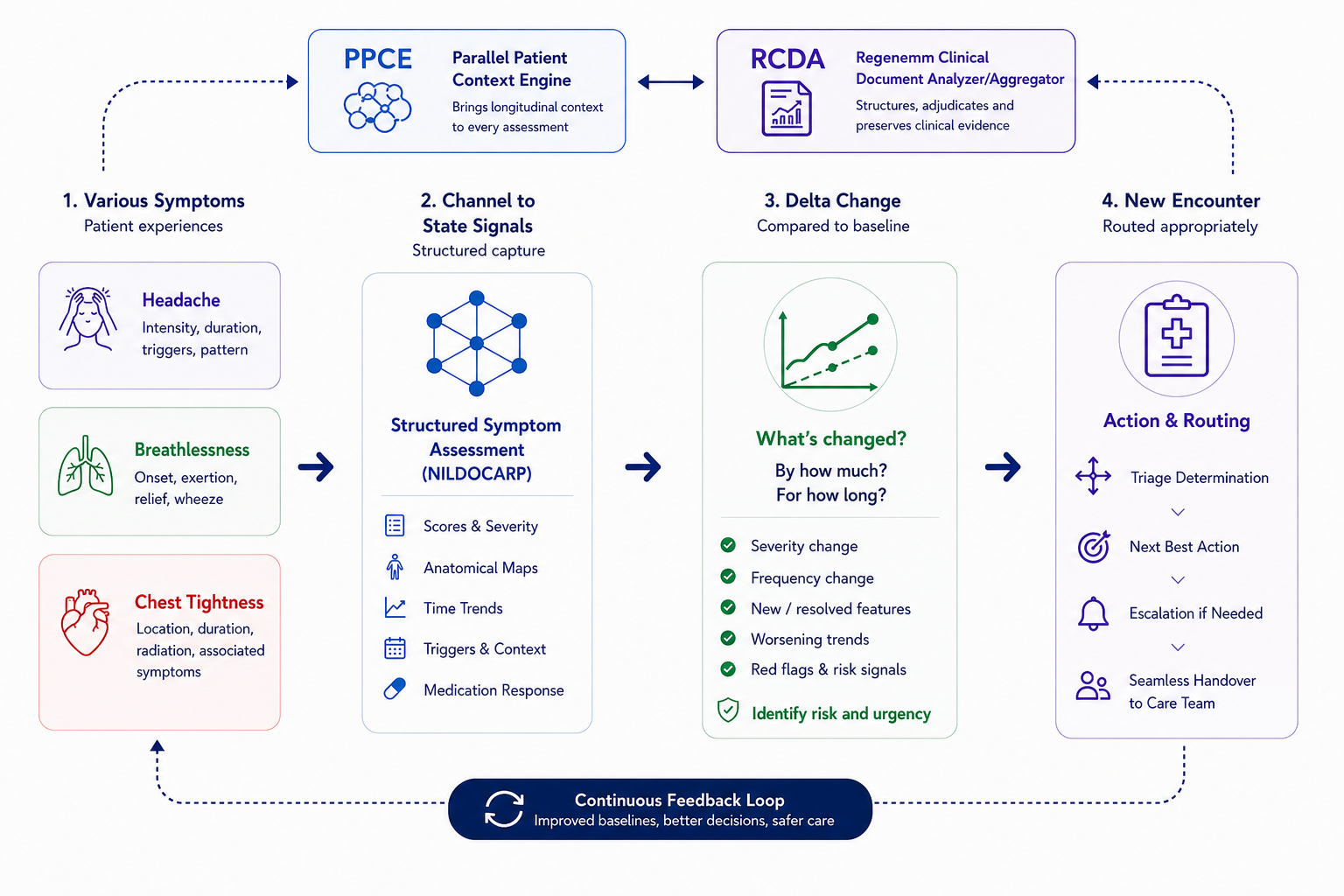
For Regenemm, this matters because structured symptoms can become part of the broader clinical state architecture. Regenemm Triage can use structured symptom signals to help identify risk, urgency, and the most appropriate next step. It does not replace clinical judgement. It helps organise the patient's symptom pattern so concerning changes are easier to recognise.
The PPCE, the Parallel Patient Context Engine, is Regenemm's longitudinal context layer. It helps compare the patient's current symptom pattern with their prior history, baseline function, previous investigations, medications, unresolved clinical issues, and known care context. In simple terms, it helps answer: how is this symptom different from this patient's usual state?
The RCDA, the Regenemm Clinical Document Aggregator, is Regenemm's clinical documentation and adjudication layer. It helps structure encounter evidence, preserve provenance, retain prior clinician-led impressions, and support current, real-time, clinician-reviewed outputs. In simple terms, it helps turn the encounter into an auditable clinical record of what changed, what was considered, and what action is required.
Symptoms and signs become more than complaints. They become governed signals of change.
And when patients, and clinicians for that matter, are given better tools to describe change, the healthcare system receives better evidence of what is changing, why it may matter, and what should happen next.
Closing
Patients are not poor historians. Clinicians are not poor observers. However, both may often be asked to tell clinically important stories without enough structure.
When patients are given better symptom tools, they can describe their condition more accurately, more consistently, and in a way that better supports clinical reasoning.
This is not merely intake paperwork. It is part of clinical state management.
The patient's subjective experience is preserved, but it is also structured, scored, mapped, compared, and interpreted.
That is how symptoms become state signals. That is how patient experience becomes safer clinical evidence.
And that is how a healthcare system begins to understand change before it becomes crisis. This is led by clinicians, not by AI assistants.